Validation
A Consistent, Accurate Body Composition Alternative to DXA
Validation of Prism's mobile 3D body scanner across 550 subjects: body fat r = 0.950 vs. DXA, plus circumference, BMI, lean mass, and visceral fat accuracy.

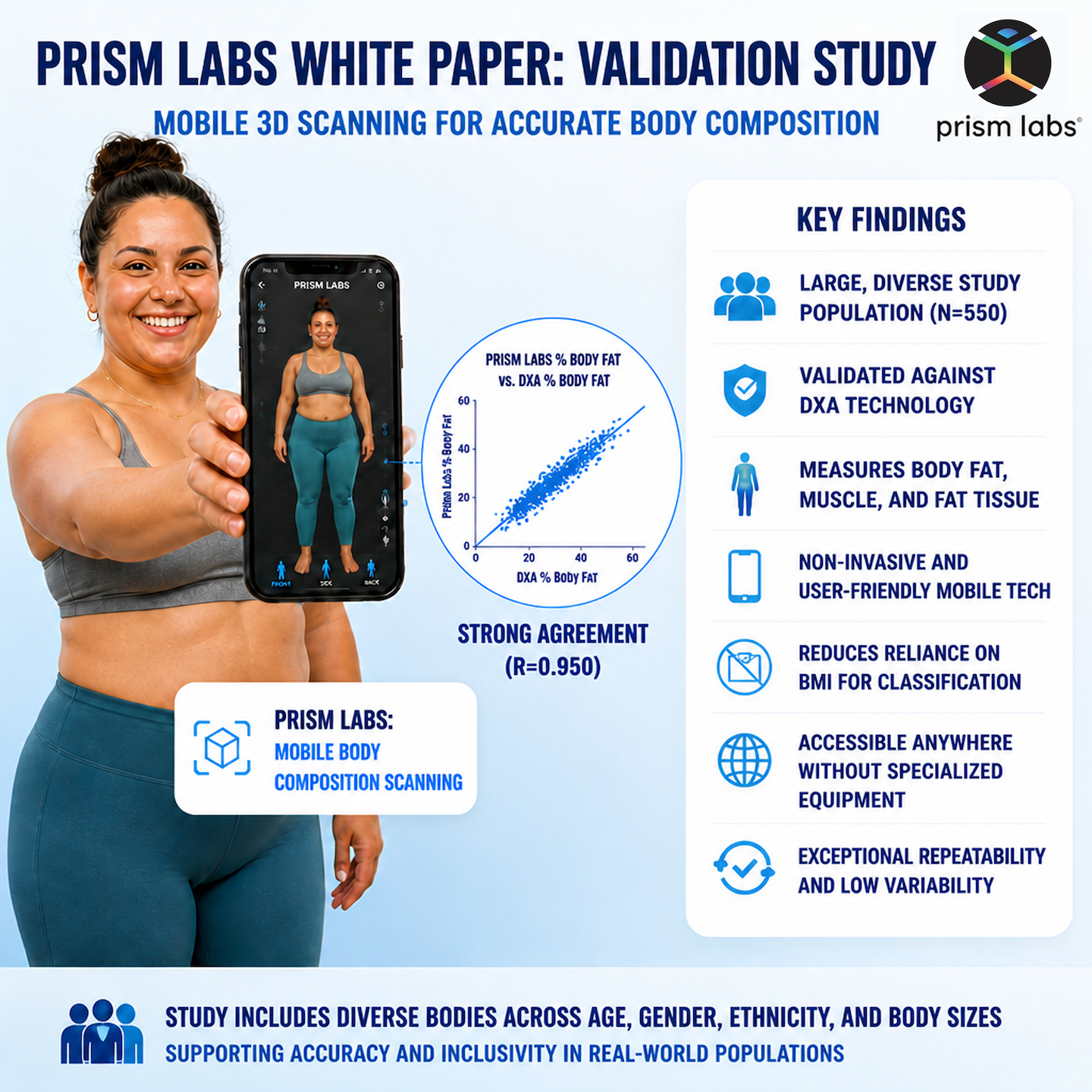
Prism Labs has developed a mobile 3D body imaging solution that delivers consistent, accurate body composition measurements from any smartphone or tablet. This validation study reports on the accuracy of Prism's scanner across 550 subjects and 3,721 scans, validated against DXA as the gold standard for body composition. Key findings include body fat percentage accuracy of MAE = 3.24% and r = 0.950 (Adaptive Model), strong agreement on appendicular lean mass (r = 0.850), skeletal muscle mass (r = 0.847), and visceral adipose tissue (r = 0.837). Within-subject scan-to-scan consistency is exceptional, with circumference measurement repeatability of 0.27–0.81 cm.
Obesity is one of the most prevalent chronic conditions in the United States and other western nations. Obese individuals face significantly elevated risk of cardiovascular disease, type 2 diabetes, and many cancers (Graf et al., 2016; Barry et al., 2014). Conversely, adequate skeletal muscle mass is associated with reduced risk of chronic disease and mortality (Lee et al., 2018; Spahillari et al., 2016; Li et al., 2018). Accurate, accessible assessment of both fat and muscle mass is therefore vitally important across the healthcare and fitness industries.
Body Mass Index (BMI), a height-and-weight formula more than 100 years old, remains the primary clinical proxy for obesity. BMI was adopted in the United States in the 1970s as an affordable replacement for body composition testing, which at the time required skilled professionals and expensive equipment. Unfortunately, BMI cannot distinguish fat mass from lean mass, making it prone to misclassification, particularly in muscular or athletic individuals. The equation was derived from a small sample of white European men in the late 19th century and does not account for sex or racial variation, nor the dramatic increase in global obesity since then. Even the original landmark comparison found BMI agreed with body composition measures in fewer than 33% of individuals (Keys et al., 1972). The American Medical Association (AMA) released a statement in 2023 recommending against sole reliance on BMI as a measure of health (AMA, 2023).
In contrast, direct measures of body fat percentage, lean mass, and fat distribution provide much stronger links to health outcomes and enable more accurate, personalized health guidance.
Prism Labs has developed a mobile 3D body imaging solution that works across iOS and Android smartphones and tablets, as well as directly from any modern web browser without requiring a dedicated app. The scanner delivers consistent, accurate body circumference and body composition measurements from the comfort of home. By removing barriers such as cost, clinic scheduling, and the need for trained technicians, Prism makes clinical-quality body data widely accessible. The scanning technology employs non-rigid avatar reconstruction from serial images (~150) captured during the user's full 360° rotation, followed by parameterized body model fitting to normalize avatar pose and ensure consistent measurement locations (Tinsley et al., 2023a).
Prism's estimation of body fat percentage uses COCO2 (Compound Circumferences Only V2), a proprietary algorithm based exclusively on dimensionless body shape ratios (e.g., waist-to-height ratio) rather than absolute circumferences. This design makes the algorithm robust across a wide range of body sizes. For cases of potential overestimation in highly muscular individuals, an Overestimation Correction variant (COCO2-OC) is also provided. Prism additionally estimates appendicular lean mass (AL), skeletal muscle mass (SM), and visceral adipose tissue (VAT) from circumference-derived features. Independent validation studies have confirmed high reliability of circumference measurements (Tinsley et al., 2023a) and strong agreement of body fat estimates with DXA (Tinsley et al., 2024a; Florez et al., 2024).
This white paper reports the accuracy and consistency of the Prism mobile scanning technology across:
The validation dataset comprises 3,721 scans from 550 unique subjects collected across ten study campaigns between 2023 and 2026. Table 1 summarizes demographics for the full dataset and the DXA-validated subset.
Circumference accuracy was assessed against measurements collected with the Naked Labs scanner, a calibrated at-home 3D body scanner, available for 78 subjects (432 scans) from two of the ten studies in the dataset.
Body composition accuracy was assessed against Dual-Energy X-ray Absorptiometry (DXA) as the gold standard. DXA provides a single reference value per subject. For accuracy analysis, Prism estimates were averaged across all available scans for each subject before comparison to the DXA reference.
BMI (calculated from user-entered weight and height) serves as the reference for BMI Estimated.
Accuracy is reported using the following metrics, computed at the per-subject level (mean estimate over all scans per subject vs. single reference value):
Consistency is reported as the within-subject standard deviation of repeated scan estimates, averaged across all subjects with two or more scans (n = 437 subjects, 3,446 scans).
All body composition metrics are reported as percentages (% body weight). Circumference measurements are in centimeters.
Three COCO2 variants are evaluated for body fat %:
It is important to note that in a real-world deployment the ground-truth DXA reference is not available, so the adaptive selection cannot be made automatically based on the outcome. In the current implementation, switching to COCO2-OC corresponds to an explicit user-activated "Athlete Mode," intended for highly muscular individuals who are aware that standard circumference-based estimates may overestimate their body fat. To guide appropriate selection, Prism provides partners with heuristics that proxy athletic body composition — such as brief screening questions on training frequency and resistance training history, or thresholds on derived anthropometric ratios (e.g., fat-free mass index from initial scan output). Partners can incorporate these into onboarding flows to route users toward the appropriate model. Prism is concurrently developing an AI-powered automatic athlete detection feature that will identify these cases from scan data alone, enabling seamless model selection without requiring user input or upstream questionnaires. This capability is expected to enter production in the near future.
Table 2 reports per-subject accuracy for all twelve body circumference sites, with the calibrated at-home 3D body scanner as the reference. This system used 3 depth cameras as input to the reconstruction. Values are averaged per subject before computing error statistics.
All measurements show a small negative bias (Prism tends to measure slightly smaller than the at-home 3D body scanner), ranging from −0.19 cm (right calf) to −1.61 cm (shoulder). The largest absolute errors are observed for shoulder and thigh measurements, while the smallest errors are seen for calf and neck measurements. Relative MAE ranges from 1.41% (hips) to 3.77% (mid-arm right). These results are consistent with external validation studies using Prism's scanner: Tinsley et al. (2023a) reported precision errors of 0.4–0.8 cm across circumference sites in 69 subjects, and McCarthy et al. (2024) found strong agreement between 3D-derived and tape-measured waist and hip circumferences (R² = 0.97) in a diverse sample of 44 adults — concluding that smartphone-based 3D scanning now achieves the accuracy required for metabolic disease-risk phenotyping at scale.
Table 3 reports within-subject standard deviation of repeated scan estimates across 437 subjects with two or more scans. The consistency analysis captures purely the Prism scanner's repeatability, independent of the reference device.
Consistency is exceptional across all body sites, with within-subject standard deviations of 0.27–0.81 cm. Distal limb segments (calf, mid-arm) show the lowest variability, while proximal trunk sites (shoulder, chest) show slightly higher variability, consistent with the expectation that limb segments are more geometrically stable across repeated measurement sessions. These within-subject SDs compare favorably to the precision errors reported by Tinsley et al. (2023a), who found a technical error of measurement averaging 0.5 cm across common body circumferences using the same non-rigid avatar reconstruction approach, noting this was lower than errors from traditional non-portable 3D scanning booths.
BMI Estimated is a circumference-based estimate of BMI that does not rely on user-entered weight or height. It is a purely anthropometric estimation derived from the 3D body scan. This provides an independent, operator-free estimate of BMI that can be useful when anthropometric inputs are unavailable, unreliable, or unavailable.
The reference ("true" BMI) is computed as weight (kg) / height (m)². Since weight and height are operator-entered values that remain essentially constant across repeat scans for the same subject, BMI itself has very low within-subject variability (mean SD = 0.05 kg/m²). BMI Estimated, by contrast, varies across scans as it is derived from scan data, with a within-subject SD of 0.29 kg/m².
Table 4 reports accuracy metrics for BMI Estimated vs. true BMI across all 550 subjects. The estimator demonstrates strong agreement overall (r = 0.945), with a near-zero mean bias (+0.06). MAE is 1.40 kg/m² and RMSE is 1.83 kg/m², with comparable performance for male and female subjects.
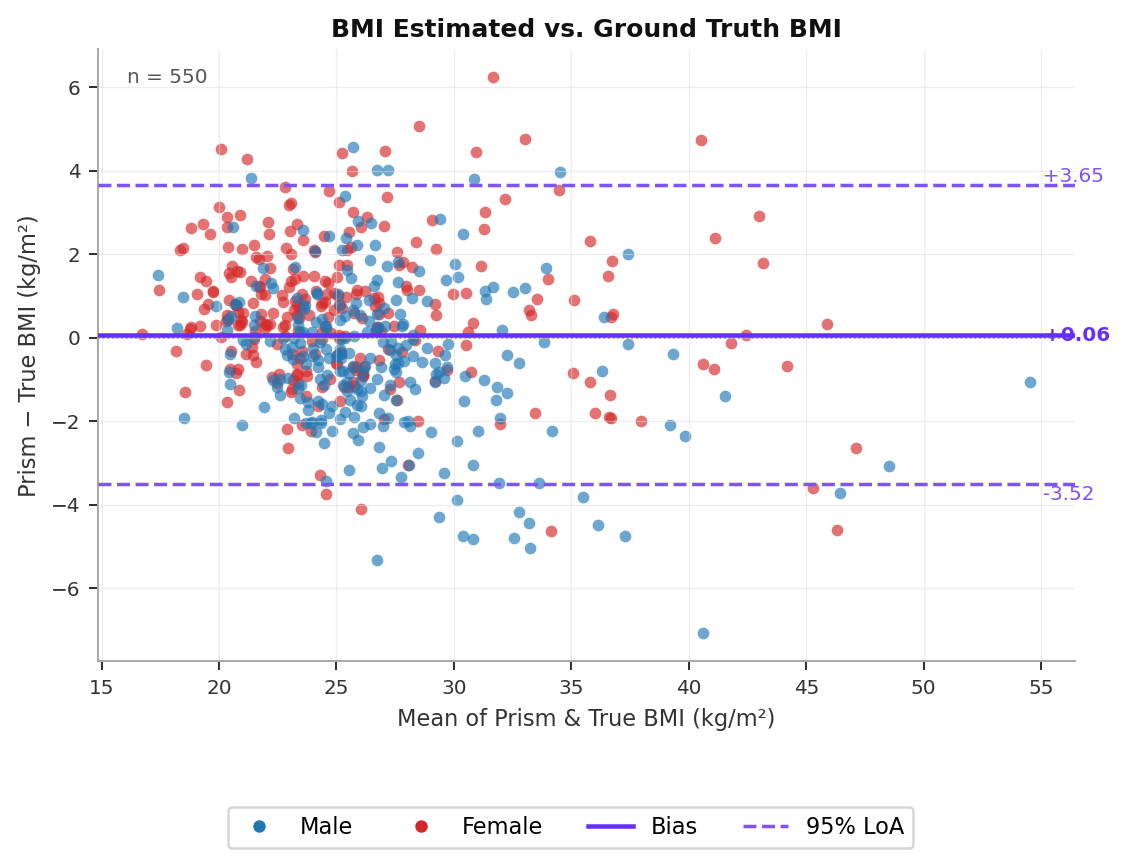
Table 5 reports within-subject consistency. BMI Estimated achieves a mean within-subject SD of 0.29 kg/m², reflecting the high scan-to-scan repeatability of the circumference measurements from which it is derived.
Table 6 reports accuracy for all three body fat estimation variants across the 273 subjects with valid DXA measurements. Results are provided overall and stratified by sex.
COCO2 Standard performs well across the full population (MAE = 3.96%, r = 0.898) and represents the primary estimator. COCO2-OC, when applied universally, underperforms (MAE = 7.01%) because it introduces a systematic negative bias in subjects for whom no correction is needed. The Adaptive Model achieves the best overall performance (MAE = 3.24%, r = 0.950), by selectively applying COCO2-OC only in the 57 subjects (21%) where COCO2 substantially overestimates DXA. For these subjects, uncorrected COCO2 overestimates DXA by a mean of +5.22 percentage points, while COCO2-OC reduces this to −0.45 percentage points. These performance levels are consistent with independent external validations: Tinsley et al. (2024a) reported MAE of ~3.4–3.5% and r = 0.90 vs. DXA in 131 subjects across two laboratory sites, with no proportional bias observed, a key indicator of equation quality. Florez et al. (2024) further demonstrated the utility of Prism-derived circumferences for body fat estimation in a population reflective of military recruits (n = 96).
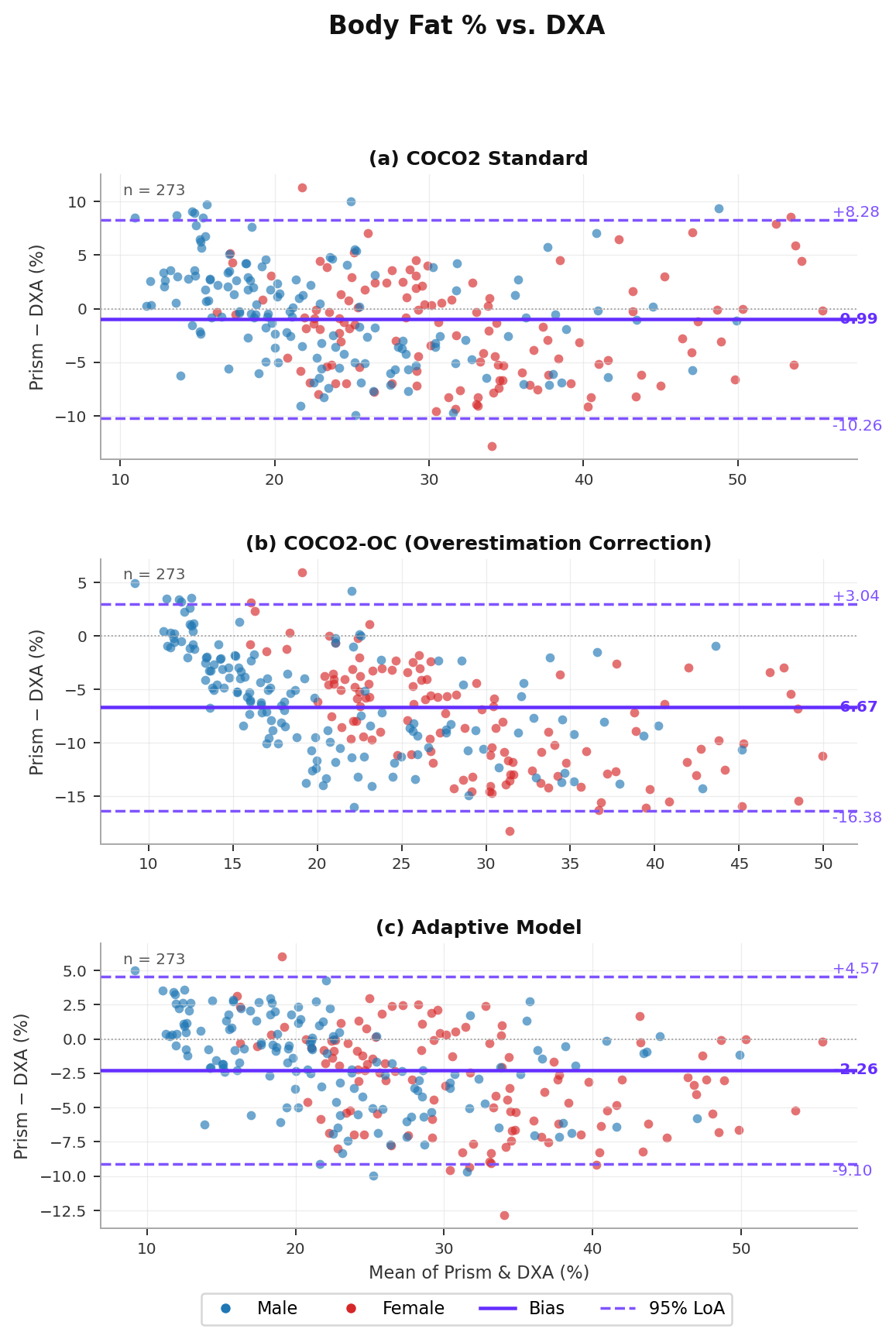
Table 7 reports within-subject consistency for all body composition metrics. Body fat % (COCO2) achieves a mean within-subject SD of 0.58%, while COCO2-OC is slightly more consistent at 0.41%. Lean mass and VAT estimators show even lower scan-to-scan variability.
In addition to body fat percentage, Prism estimates three further body composition metrics from circumference-derived features:
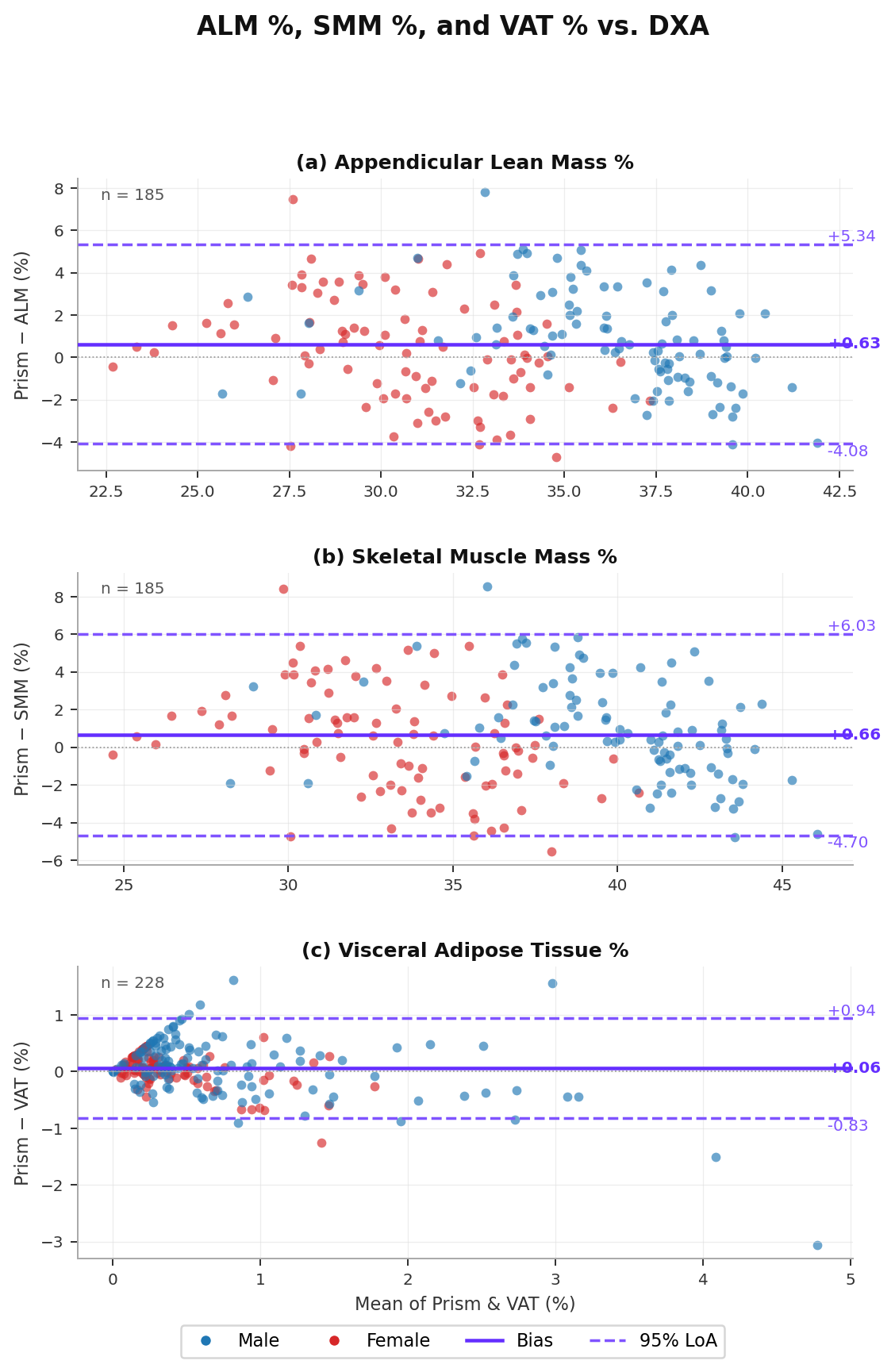
DXA provides a single per-subject reference value for each metric. Prism estimates are averaged per subject across all available scans. Valid DXA reference data is available for 185 subjects (ALM, SMM) and 228 subjects (VAT).
Table 8 reports per-subject accuracy for all three metrics, overall and stratified by sex.
Both ALM and SMM show a small positive bias (+0.62% and +0.66% respectively), indicating a slight tendency to overestimate lean mass relative to DXA. MAE is 1.97% for ALM and 2.23% for SMM, with correlations of r = 0.850 and r = 0.847 respectively.
VAT is estimated with the highest relative accuracy, showing near-zero mean bias (+0.06%) and MAE of 0.31%, with r = 0.837. Male subjects show slightly higher VAT errors than female subjects, consistent with known sex differences in visceral fat distribution patterns. The clinical relevance of Prism's waist circumference measurements for VAT prediction is further supported by McCarthy et al. (2024), who showed that 3D-derived waist circumference predicts DXA-measured VAT mass as accurately as manual tape measurement (R² = 0.70 vs. 0.69), including when stratified by sex.
The Prism mobile scanner demonstrates exceptional scan-to-scan consistency across all body circumference sites, with within-subject standard deviations of 0.27–0.81 cm. This makes repeat measurements reliable enough to track meaningful body shape changes over time. Accuracy against the calibrated at-home 3D body scanner is strong, with mean absolute errors of under 0.9 cm at the calf and 1.5 cm at the hips, site sizes at which measurement variability in manual tape measurements is typically comparable or greater. These findings are reinforced by independent precision data (Tinsley et al., 2023a) and external accuracy studies demonstrating strong agreement with trained-anthropometrist tape measurements for waist and hip circumferences (McCarthy et al., 2024).
A circumference-derived BMI estimate is now available from the Prism scanner, enabling BMI assessment without requiring user-entered weight and height. With MAE of 1.40 kg/m² and r = 0.945 across 550 subjects, this estimator provides a reliable independent proxy for BMI, and is particularly valuable in clinical or research settings where operator-entered anthropometrics may be unavailable.
COCO2 provides accurate body fat percentage estimates with MAE = 3.96% and r = 0.898 vs. DXA across a diverse dataset of 273 subjects. The Adaptive Model further improves performance (MAE = 3.24%, r = 0.950) by applying the overestimation correction selectively for the ~21% of subjects where COCO2 substantially overestimates DXA. This approach is recommended in production as it reduces systematic bias in highly muscular individuals while preserving accuracy for the general population. Independent external validation by Tinsley et al. (2024a) reported comparable overall accuracy (MAE ~3.4–3.5%, r = 0.90, no proportional bias), and equivalence testing confirmed statistical equivalence with DXA within ±2.0% BF% bounds, establishing the clinical acceptability of the estimator. In the current implementation, activation of the overestimation correction corresponds to a user-initiated Athlete Mode. Prism is developing an AI-powered automatic detection feature that will identify high-muscular subjects from scan data alone, enabling model selection without any user input; this is expected to enter production in the near future.
Prism's estimates of appendicular lean mass %, skeletal muscle mass %, and visceral adipose tissue % are each validated against DXA, showing correlations of r = 0.837–0.850. These metrics extend Prism's clinical utility beyond a single fat percentage number to a more complete body composition profile, enabling clinicians and users to track changes in muscle mass and visceral fat independently. McCarthy et al. (2024) further demonstrated that Prism-derived waist circumference and waist-to-hip ratio are equally predictive of visceral adipose tissue as tape-based measurements, supporting the clinical utility of digital anthropometry for metabolic disease-risk phenotyping.
Taken together, these results demonstrate that the Prism mobile scanner provides a consistent, accurate, and accessible method for body composition assessment. By enabling DXA-comparable measurements in a home setting, without skilled technicians, specialized equipment, or radiation exposure, Prism substantially lowers the barriers to regular body composition monitoring for both clinical and consumer use cases. The availability of native iOS and Android apps alongside a browser-based version means these capabilities are accessible regardless of device or platform.
Weight management and metabolic health applications represent a particularly important use case for Prism. Individuals with obesity (BMI ≥ 30 kg/m²) are disproportionately affected by conditions such as type 2 diabetes, cardiovascular disease, and metabolic syndrome, and stand to benefit most from accessible, high-frequency body composition monitoring. Standard DXA-based assessments are often impractical in this population due to cost, radiation exposure, and equipment weight limits, making a validated mobile alternative particularly valuable.
This appendix reports accuracy metrics for BMI Estimated and all body composition outcomes (body fat %, ALM %, SMM %, and VAT %) restricted to the subset of subjects with a true BMI ≥ 30 kg/m² (n = 93 subjects, 51 male / 42 female; BMI range 30.1–55.1, mean 36.0 ± 5.3 kg/m²). Circumference measurement accuracy is not reported separately for this subset, as the primary circumference validation was conducted against a reference scanner and is not stratified by BMI. The same per-subject averaging methodology and exclusion criteria (excluding measurements with values of −1) apply as in the main analysis.
Table A1 reports accuracy for BMI Estimated in the obese subset. The estimator maintains reasonable agreement (r = 0.897), with a slight negative bias of −0.96 kg/m² and MAE of 2.06 kg/m² — modestly higher than in the full population, reflecting the greater anatomical variability in individuals with obesity. Female subjects show near-zero bias, while male subjects show a larger negative bias of −1.81 kg/m².
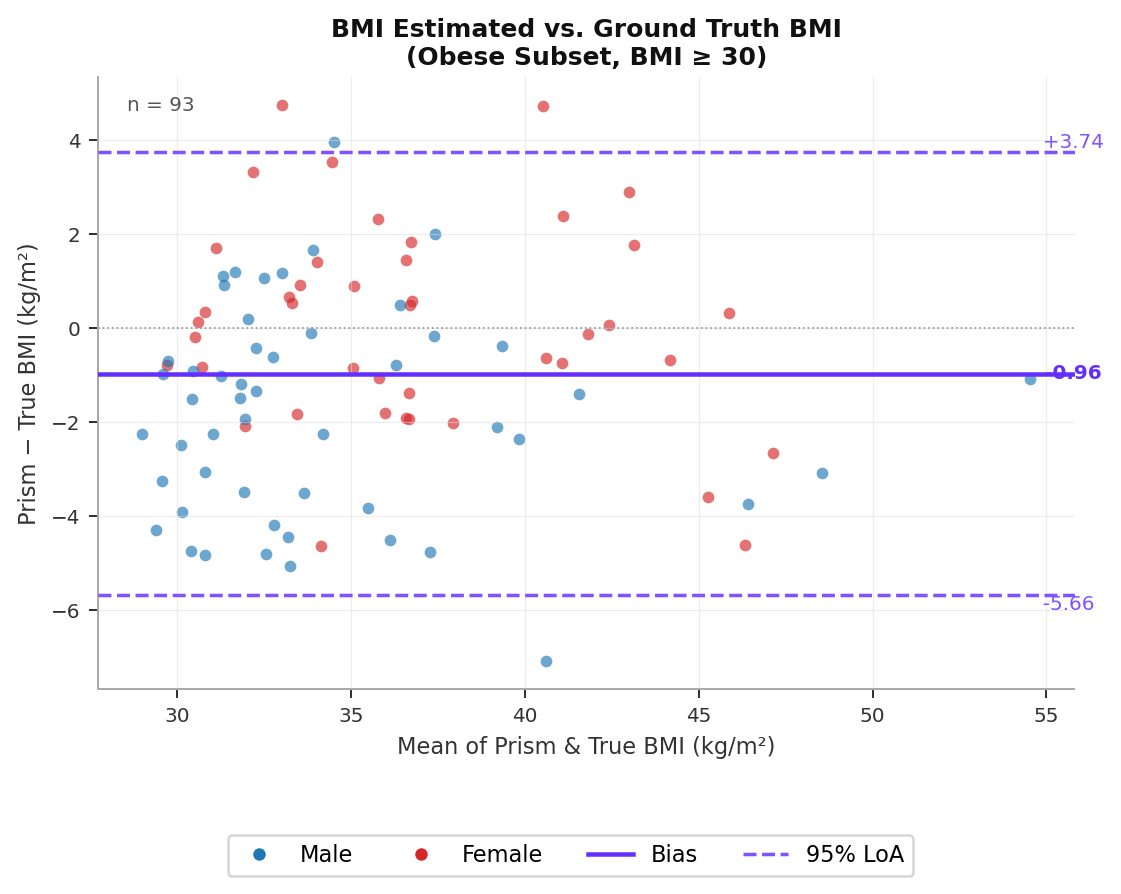
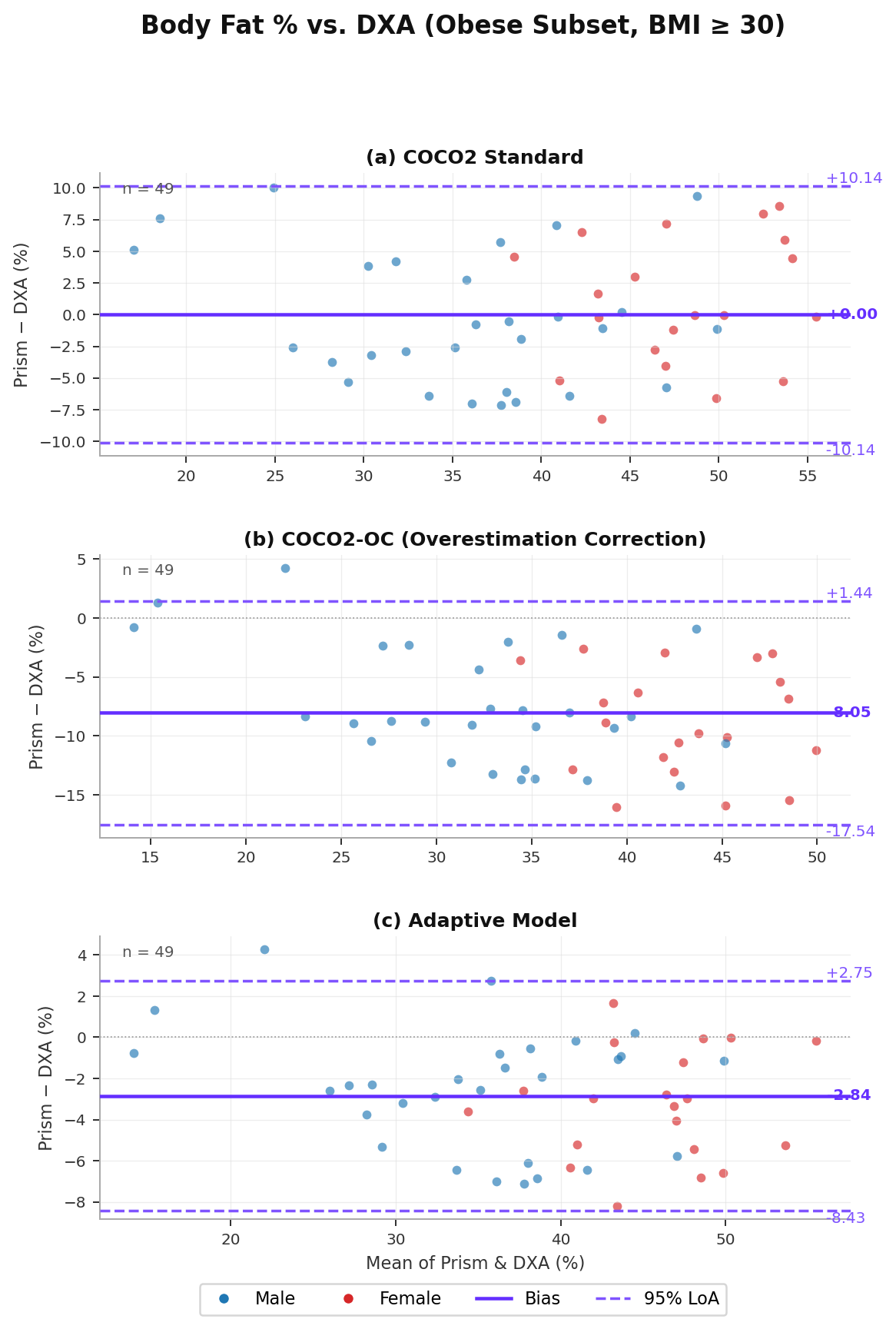
Table A2 reports body fat % accuracy for the obese subset across all three model variants. COCO2 shows near-zero mean bias (+0.00%) in this population, with MAE of 4.31% and r = 0.853, indicating the estimator performs well without systematic over- or underestimation. The Adaptive Model again achieves the best overall performance (MAE = 3.26%, r = 0.954), with 16 of 49 subjects (33%) routed to COCO2-OC — a higher proportion than the full dataset (21%), consistent with the expectation that obese individuals are more likely to exhibit circumference distributions that trigger the overestimation correction. The LoA for the Adaptive Model are [−8.43, +2.75]%, reflecting tighter upper bounds compared to the full dataset.
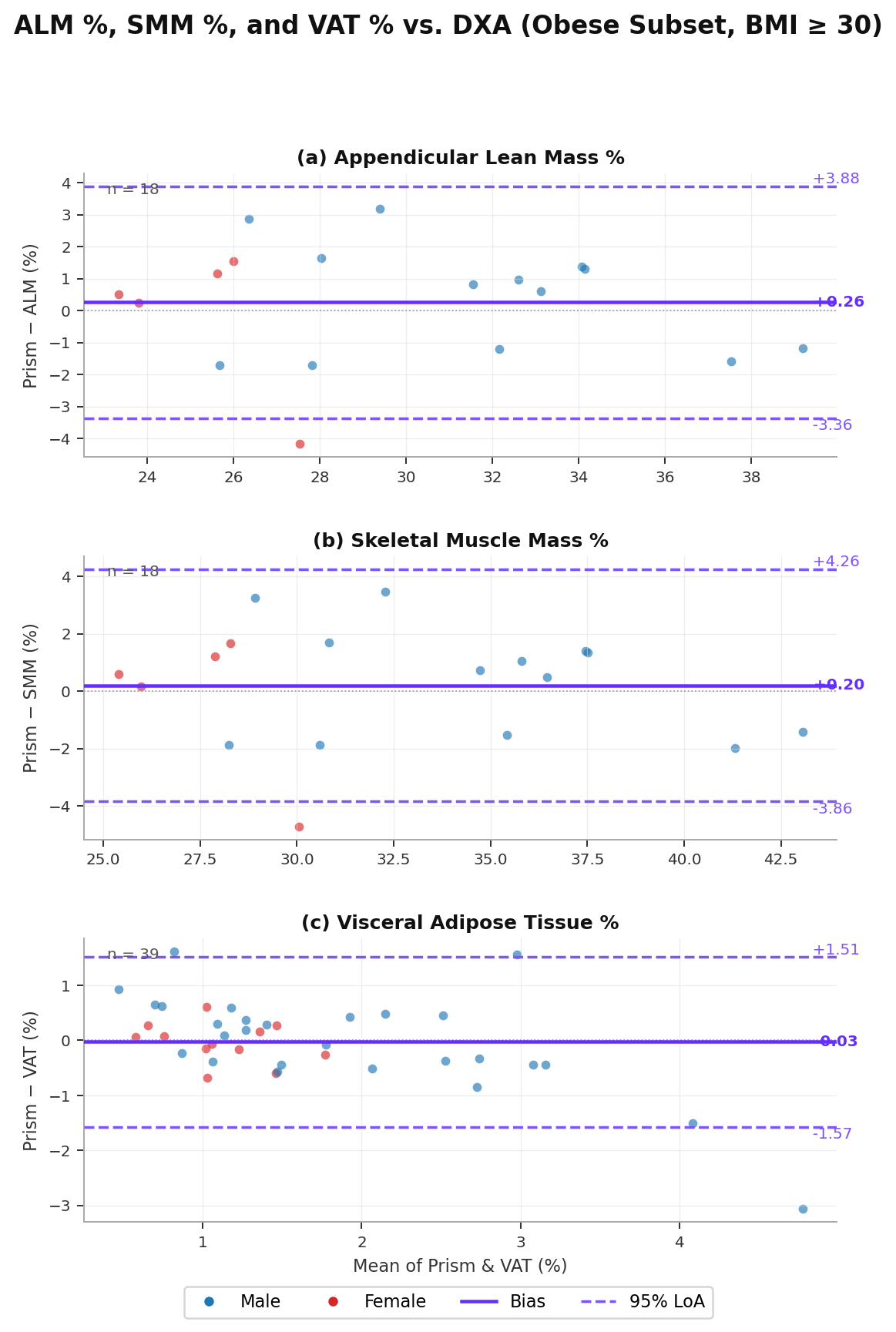
Table A3 reports accuracy for ALM %, SMM %, and VAT % in the obese subset. ALM and SMM show improved correlations (r = 0.924 for both) and reduced bias compared to the full dataset, suggesting the lean mass estimators are well-calibrated in this population. The DXA subset for these metrics is smaller (n = 18 for ALM/SMM, n = 39 for VAT) as lean mass DXA measurements were available only from specific study campaigns. VAT accuracy shows somewhat wider limits of agreement ([−1.57, +1.51]%) relative to the full dataset, reflecting the greater heterogeneity in visceral fat distribution patterns in individuals with obesity. Overall, these results support the clinical applicability of Prism’s body composition metrics specifically in the obese population.
Full reference list with citations to Tinsley et al. (2023a, 2023b, 2024a), Florez et al. (2024), McCarthy et al. (2024), and others available in the downloadable PDF.